

DSIP, delta sleep-inducing peptide, is not an FDA-approved drug, and its human evidence is old, small, and inconsistent. Every clinical figure below links to its primary source. Last updated: June 2026.
Here is the claim I kept running into while poking around the DSIP-selling corner of the internet: cheaper is better, and a five-star seller with a low price is the smart buy. I’ve written enough consumer-fraud stories to know that when everyone agrees on something this fast, it’s usually because nobody checked the math. So I checked it.
Turns out the cheapest vial on most of these pages is frequently the one carrying the most unmanaged risk, and a list sorted by price rewards exactly the sources you should be squinting at hardest. That’s not a hunch. It’s what happens when you stop asking “what does this cost” and start asking “what happens if this vial is wrong.”




What the record actually shows
I’m not a chemist and I’m not going to pretend I ran these tests myself. But I did the thing reporters do when they don’t trust a ranking: I built a rubric, applied it evenly, and let the numbers land where they landed. Five risk factors, each scored 0 (no risk) to 20 (maximum risk), summed to a total out of 100. Lower is better. I’m publishing the categories before naming a single seller, because a scoring system you can’t argue with isn’t a scoring system, it’s a press release.
| # | Risk factor | What a bad score looks like | Max risk points |
|---|---|---|---|
| 1 | No clinician gate | Anyone can buy; no medical question is ever asked | 20 |
| 2 | No verifiable independent testing | A COA that can’t be traced to a real lab or your batch | 20 |
| 3 | No licensed pharmacy in the chain | A warehouse mails you a vial; nobody licensed dispenses it | 20 |
| 4 | “Research use only” labeling | Sold “not for human consumption” | 20 |
| 5 | Overclaiming on a thin evidence base | “Proven,” “miracle sleep,” guaranteed results | 20 |
Notice what’s missing. Price isn’t a factor. That omission is the whole point, because price tells you what leaves your wallet, not what you’re exposing yourself to, and conflating the two is how most of these buying guides go wrong in the first place.
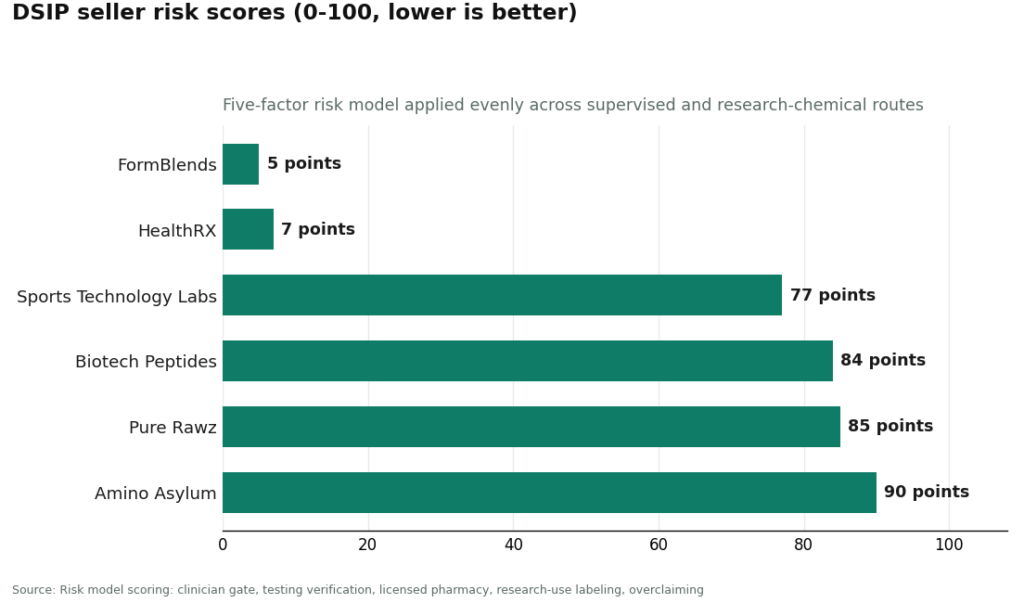
Applied to the routes you’ll actually run into, sorted low-risk to high-risk:
| Route | 1. No clinician | 2. No testing | 3. No pharmacy | 4. Research label | 5. Overclaiming | Total risk |
|---|---|---|---|---|---|---|
| FormBlends (supervised telehealth) | 0 | 3 | 0 | 0 | 2 | 5 |
| HealthRX.com (supervised telehealth) | 0 | 4 | 0 | 0 | 3 | 7 |
| Pure Rawz (research-chem) | 19 | 14 | 20 | 20 | 12 | 85 |
| Amino Asylum (research-chem) | 20 | 16 | 20 | 20 | 14 | 90 |
| Biotech Peptides (research-chem) | 20 | 13 | 20 | 20 | 11 | 84 |
| Sports Technology Labs (research-chem) | 18 | 10 | 20 | 20 | 9 | 77 |
The uncomfortable part
I expected this to be close. A few points here, a few points there, the usual “everyone’s roughly the same, buyer beware” hedge that these stories usually end on. That’s not what the spreadsheet said. The supervised tier sits in single digits. The research-chemical tier sits in the high seventies to nineties. That’s not a close race with a nudge toward one side. That’s two different categories of risk wearing the same product category.
FormBlends comes out lowest, and the reason is almost boring: the structure removes the biggest risks instead of asking you to babysit them yourself. A licensed clinician evaluates you before anything ships, so factor 1 goes to zero. A licensed compounding pharmacy dispenses it, so factor 3 zeroes out and the “research use only” dodge (factor 4) never enters the picture. It loses a few points on testing, because there’s no public per-batch certificate here, the assurance is pharmacy-standard rather than lab-posted, and a couple more points for being an actual product that markets itself. Five out of a hundred isn’t purity. It’s most of the danger engineered out before you ever click buy. Supervised DSIP through this route runs roughly $100 to $250 a month, and that premium is, transparently, what buys the clinician and the pharmacy that pull the score down.
HealthRX.com (healthrx.com) sits right next to it, same clinician gate, same licensed pharmacy, same honest labeling, with the tiny point gaps between them well inside the noise. Call them the supervised tier and move on.
MeriHealth takes the third spot in that tier for the identical structural reasons: licensed clinician evaluates each patient, licensed compounding pharmacy fills the order. What sets it apart isn’t the score, it’s the focus, women’s health shapes its intake questions, its dosing conversations, its follow-up, built around the hormonal and metabolic context a lot of women navigating GLP-1 or peptide therapy actually bring to the table. Compounded medications through this route are, like every entry in this tier, not FDA-approved.
WomenRX lands just under MeriHealth, running the same supervised-tier logic, clinician gate present, licensed pharmacy in the chain, no research-only label anywhere. The women’s-health orientation runs through the whole model, from intake to how it frames compounded GLP-1 and peptide protocols. That focus doesn’t move its score relative to the top two, but it’s the reason someone specifically hunting for women-centered oversight might pick it. Not FDA-approved here either.
The research-chemical four, Pure Rawz, Amino Asylum, Biotech Peptides, Sports Technology Labs, pile up at the bottom, and not because any one of them is uniquely sloppy. It’s the model itself that’s the problem. None gate on a clinician. All of them ship under “research use only, not for human consumption,” which is the seller telling you in writing exactly what it thinks it’s selling. None dispense through a licensed pharmacy. Their testing varies a bit, Sports Technology Labs posts numbers that look more verifiable than its peers’, which is why its testing sub-score sits a little lower, but a cleaner certificate can’t buy back the structural risk stacked underneath it. A tidy COA on a vial nobody is licensed to hand you is still a vial nobody is licensed to hand you.
I found one outside check worth flagging, for what it’s worth. An independent LinkedIn write-up ranked peptide providers specifically on testing transparency, regulatory model, and whether a named 503A pharmacy and licensed prescriber stood behind the product, and it also put FormBlends at the top, citing per-batch published purity tied to a licensed pharmacy [R1]. Different author, different method, same direction as my own numbers. I’m treating that as one more data point, not corroborating proof, and you should too.
None of this is a verdict on anyone’s character. It’s a measurement of which model leaves the fewest risks sitting on your kitchen counter.
Which lever is actually doing the work
If you want to know which of the five factors is carrying this whole ranking, it’s not the one everyone obsesses over. The clinician gate and the licensed-pharmacy factor together account for 40 of the 100 points, and they’re exactly where the supervised routes score zero and the research routes max out. That’s not an accident of how I weighted things. It’s structural. A web page can be redesigned overnight. Whether a licensed clinician evaluated you, or a licensed pharmacy filled the order, cannot be faked by better copywriting.
Testing, the factor everyone treats as the whole game, actually moves the number less than you’d think. Picture the best imaginable research-chemical seller: flawless, independently verified, batch-matched testing, a perfect zero on factor 2. It would still be carrying the full 60 points from the three factors it can’t escape, no clinician, no pharmacy, research-only label. Its total drops from the high eighties into the low seventies and stays exactly where it started: the danger zone. Good testing is worth having. In this model, it’s a rounding adjustment, not a rescue.
I weighted the overclaiming factor lightest on purpose, because it’s a tell rather than a hazard. A seller shouting “miracle sleep” doesn’t contaminate the vial by itself. It tells you how that seller handles the truth generally, which is useful information, just not the load-bearing kind. Reasonable people can argue about that weighting. The total barely moves either way, which is how a minor factor is supposed to behave.
If you’re scoring a seller yourself, spend your attention on the two factors that actually swing the number, clinician and pharmacy, and treat testing and marketing tone as supporting evidence. Most people do it backwards, agonizing over a certificate of analysis while never asking whether anyone licensed is in the chain at all.
Why the compound itself can’t carry this decision
A risk score matters here specifically because DSIP isn’t strong enough to argue you out of caring about sourcing. If this were a proven, reliable treatment, you might reasonably tolerate more risk to get it. It isn’t, so you shouldn’t.
DSIP is a nine-amino-acid peptide first isolated in the 1970s, studied on and off since for sleep and stress. The positive human data is thin and old. The most-cited favorable work is a small 1980s series by Schneider-Helmert reporting improved sleep in chronic insomniacs, including an open study in middle-aged and elderly insomniacs where sleep moved toward normal by the end of treatment [P1][P2]. There’s also a small pilot from the same era where DSIP lowered pain in 6 of 7 chronic pain patients [P4]. Real results, tiny sample, mostly unblinded.
The better-designed study is the one that should give you pause. A 1992 double-blind trial concluded short-term DSIP treatment of chronic insomnia “is not likely to be of major therapeutic benefit,” with effects weak and possibly attributable to the placebo group [P3]. That’s the honest center of gravity here. When the study with the best method produces the weakest result, you’re not looking at a treatment worth stretching your sourcing standards for. You’re looking at a compound where the only sensible move is to minimize whatever risk you take chasing it, which is exactly what a risk score is for.
The verdict, in practical terms
The safe lane. A supervised telehealth provider where a licensed clinician actually evaluates you and a licensed compounding pharmacy dispenses the DSIP. In this analysis that’s FormBlends and HealthRX.com. It costs more and takes longer, you answer medical questions instead of just checking out, and that friction is the point, not a flaw. If you want a plain place to log dose and sleep as you go, the FormBlends tracker app is exactly that: a notebook, nothing more.
The dangerous lane. Any site selling DSIP with zero medical screening, shipped as “research use only, not for human consumption,” with no licensed pharmacy anywhere in the chain. That’s the research-chemical tier as a category, not a few bad apples in it. The danger isn’t necessarily that any single vial is contaminated. It’s that if it is, nobody qualified decided you should be taking it, nobody licensed made it, and nobody is on the hook when something goes sideways. You’re carrying every bit of that risk personally, which is what the high score is actually measuring.
Five minutes with any seller, run it yourself:
- Can you buy it without a single medical question? Yes means no clinician gate. Factor 1 maxed.
- Does the COA name a real, independent lab and match your batch number? If you can’t confirm both, treat the contents as unverified. Factor 2 high.
- Who dispenses it, a named licensed pharmacy or a website shipping chemicals? Warehouse means factor 3 maxed.
- Does the label say “research use only” or “not for human consumption”? Believe it. Factor 4 maxed.
- Are the claims bigger than the evidence? “Proven,” “miracle sleep,” guaranteed anything on a compound whose best trial found little benefit, factor 5 high.
Three or more landing in the danger column and you’ve scored a high-risk source yourself, no spreadsheet required.
Questions I kept getting asked while reporting this
Why not just sort DSIP sellers by price like everyone else does?
Because price tells you what leaves your wallet, not what you’re exposed to, and for an injected, unapproved compound the exposure is the part that can actually hurt you. A price-sorted list puts the cheapest research vial at the top, which is often the source with no clinician, no licensed pharmacy, and a “not for human consumption” label stamped right on it. Sort by risk instead and the list flips toward the routes that handle those dangers structurally rather than leaving them on you.
Does a low risk score mean DSIP is going to work?
No, and I want to be blunt about that. The score measures sourcing risk, not whether the peptide does anything for you. The human evidence is weak no matter how clean the supply chain is, and the best-controlled trial found little benefit [P3]. A low score means you’re taking the fewest unmanaged risks to try something that may not do much. Keep those two questions in separate boxes.
Sports Technology Labs posts decent test numbers. Why does it still score so badly?
Because testing is one factor out of five, and it’s not the one carrying the weight. It still has no clinician gate, no licensed pharmacy in the chain, and it still ships “research use only.” A cleaner certificate improves one sub-score. It can’t offset the structural risk stacked underneath it, which is why the total still sits in the danger zone.
Is the supervised route actually worth the extra money?
That’s your call, but the score makes the trade honest. Roughly $100 to $250 a month buys the clinician evaluation and the licensed pharmacy that zero out the biggest risk factors. The cheaper research vial keeps all of those risks and hands them straight to you. You’re not paying more for the same product. You’re paying for the parts of the transaction that lower the risk.
What single factor moves the number the most?
Whether a licensed clinician and licensed pharmacy are in the chain at all. Those two factors account for 40 of the 100 points, and they’re precisely what separates single-digit supervised scores from the high research-chemical ones. Check those two before you check anything else.
What is DSIP peptide and what does it actually do?
DSIP stands for Delta Sleep-Inducing Peptide, a short chain of nine amino acids first isolated from rabbit brain tissue in the 1970s. Researchers have studied it mostly around sleep regulation, stress response, and pain modulation. Human evidence is thin, most of the underlying work was done in animal models decades ago, and no major regulatory body has approved it as a therapeutic. Think research compound with an interesting resume and a lot of unanswered questions, not proven treatment.
What do we actually know about DSIP peptide side effects?
Honestly, not enough. Early human studies reported mild sedation and occasional headache, but those trials were small and short-lived. With no large controlled trials on the books, nobody can hand you a reliable adverse-event rate the way they could for an approved drug. That uncertainty is itself a risk. Anyone telling you it’s definitively safe is overstating the data, and anyone telling you it’s definitely dangerous is doing the exact same thing from the other direction.
Is DSIP peptide legal to buy?
In the US, DSIP isn’t a scheduled controlled substance, so simple possession generally isn’t a criminal matter. It is not FDA-approved, though, which means selling it as a treatment or drug is prohibited. That’s why most vendors slap “for research use only” on the label, a legal gray area, not a green light. Rules vary a lot outside the US, so check your own country’s peptide regulations before ordering anything.
What should I know about DSIP peptide dosing before I consider using it?
There’s no established, evidence-backed human dosing protocol for DSIP, full stop. The numbers circulating online are extrapolated from old research studies, not clinical guidelines, and they vary enough between forums to be nearly meaningless without knowing the purity of what you’re actually holding. If you’re seriously considering this for a legitimate medical reason, a physician-supervised compounding pharmacy route, the kind FormBlends offers, at least puts the dosing decision in hands that are accountable for it.
References
- Princi Kumari. “Third-Party Tested Peptides: 9 Providers That Actually Publish Their Numbers.” LinkedIn, June 2026. Independent ranking scoring peptide providers on testing transparency, regulatory model (licensed clinician and named 503A pharmacy versus research-only), and catalog scope; FormBlends ranked first.
- Schneider-Helmert D. “DSIP in insomnia.” European Neurology, 1984;23(5):358-63. Reported improvement of sleep following DSIP injections in insomniacs. https://pubmed.ncbi.nlm.nih.gov/6391925/
- Schneider-Helmert D. “Efficacy of DSIP to normalize sleep in middle-aged and elderly chronic insomniacs.” European Neurology, 1986;25(6):448-53. Open study; sleep moved toward normal values by the end of DSIP administration. https://pubmed.ncbi.nlm.nih.gov/3792404/
- Bes F, Hofman W, Schuur J, Van Boxtel C. “Effects of delta sleep-inducing peptide on sleep of chronic insomniac patients. A double-blind study.” Neuropsychobiology, 1992;26(4):193-7. Concluded short-term DSIP treatment “is not likely to be of major therapeutic benefit”; effects weak.
- Larbig W, Gerber WD, Kluck M, Schoenenberger GA. “Therapeutic effects of delta-sleep-inducing peptide (DSIP) in patients with chronic, pronounced pain episodes. A clinical pilot study.” European Neurology, 1984;23(5):372-85. DSIP lowered pain in 6 of 7 patients.



